| 333
|
CHAPTER 50
Mentally Handicapped Girls
Assist Multiply-Disabled Children:
Outcome of a CBR Training Course in Brazil
Helping Rehabilitation Professionals Listen to and Work as
Partners with Disabled Persons
Brazil is a vast country of diverse cultures and striking
contrasts. A small percentage of people are enormously wealthy. Millions
live in poverty. Big cities have a few modern, highly sophisticated
rehabilitation centers. But most disabled persons - especially those
living in shanty towns and rural areas - receive little or no assistance
beyond what their families can provide. Big barriers, both physical and
social, lie in the way of full community integration.
An effort to improve this situation is being made by CORDE, a
branch of the Ministry of Justice concerned with the integration and needs
of disabled persons. CORDE is now committed to introducing Community Based
Rehabilitation (CBR) throughout Brazil.
In November, 1996, CORDE invited me (David Werner) to the coastal city
of Recife to facilitate a one week course for future "multipliers" of CBR.
According to an early plan, most course participants were to be
rehabilitation professionals from government institutions. However,
experience in many countries has shown that many of the most
successful CBR programs are started from below by those who are most
concerned: by groups of disabled persons and families of disabled
children.
Therefore, to facilitate a partnership approach - and to open the way
for disabled persons to play a leading role in planning and implementing
CBR programs - it was decided that the course include:
- a substantial number of disabled participants (or family members),
some of whom should be disabled organization leaders and activists;
- home visits and discussions with willing, local disabled
persons/families living in difficult circumstances, to get their views
on needs, obstacles, wishes, and ideas for priorities;
- hands-on, problem-solving activities with disabled children and
their families, including making assistive devices with low-cost
materials, designed for and with the individual child.
We felt that if the course could help rehabilitation
professionals work together with communities, listen to disabled persons,
and relate to them as partners and equals in the problem-solving process,
much might be gained. The goal should be to encourage rehabilitation
workers to EMPOWER, not merely to prescribe.
The CORDE staff did a good job of recruiting. Nearly one quarter of the
course participants were either disabled themselves or were parents of
disabled children. These disabled participants - who included leaders of
disabled persons' associations, community service programs, and Brazil's
budding Independent Living Movement - provided a key dynamic. They led
discussions about needs and possibilities based on their own experiences. |
| 334
|
|
COURSE PREPARATIONS. In preparation for the course,
we facilitators visited a government-run hostel for abandoned, severely
disabled children. Sixty children were cared for by an average of only 5
or 6 caretakers at any one time. Several of the most handicapped
children appeared to be starving. Their wasted condition (marasmus) was
apparently due, not to scarcity of food, but to a shortage of staff.
Those children who had poor head-control and trouble swallowing could
take only liquid foods in small sips. Getting enough food into them
called for a lot of time and patience. With so many children to feed,
clean, and care for, the few care-providers did not have time to
adequately feed and mother those who needed extra help. As a result,
these children were becoming more and more disabled. Apart from
insufficient food, they got less hugging and stimulation than needed for
their minds and bodies to grow.
On arriving at this hostel, we saw a dozen disabled children lined up
on the porch, sitting in wheeled strollers. All the strollers were
exactly the same - regardless of the size, spastic patterns, or
individual needs of the children. Their canvas seats were held by
metal-tube frames. The children sat passively in half-reclining
positions, like sacks of potatoes.
The strollers neither provided good positioning nor stimulated head
and body control. For many of the children, the awkward positioning was
leading to increasing spasticity and deformity. A few of the less
severely disabled children were able to take a few steps with
assistance, but they had no walkers. The one walker we saw was broken.
Given these children's extensive unmet needs, it occurred to me that
- with some guidance and the use of books (such as Disabled Village
Children) - the participants in the training course might be able
to make simple, individually-adapted seats, assistive devices, and
stimulating play-things for some of the children. With the help of the
staff, we chose 6 children whom they agreed to take to a workshop to be
conducted during the course.
CHILD-TO-CHILD. One day of the course was spent on
Child-to-Child activities. Participants watched a slide-show from Mexico
to spark their imaginations. Then they practiced Child-to-Child
activities among themselves - including simulation games, role-plays,
and discussions to sensitize school-age children to the needs and
potentials of children who are different.
That afternoon, participants went to a public school. Small groups
visited different classrooms. After ice-breaking games, they facilitated
activities with the children. At first, the children were shy. But when
they discovered that the adults actually listened to them and took
interest in their ideas, the kids warmed up. They expressed their doubts
and fears concerning disability. They acted out role-plays, and asked
perceptive questions.
At the end, participants asked the children if they had liked the
activities, and what they had learned. What they liked most,
they said, was the chance to talk openly with the disabled members of
our group, some of whom were blind or paralyzed. One of our
group, Geronimo - who has flipper-like arms and marked deformities -
quickly won the children's respect with his friendliness, candor, and
self-assurance. One of their lingering doubts was put to rest when
Geronimo introduced his vivacious young wife and said they were
expecting a baby. The students agreed that the activities and
discussions helped them realize that disabled people are ordinary people
like themselves, with the same needs, emotions, and dreams. It
is what we have in common that matters most. |
| 335
|
| THE APPROPRIATE TECHNOLOGY
WORKSHOP. Two days of the course were spent in a small
wheelchair-making shop run by disabled youth in a poor neighborhood. We
facilitators had visited the shop beforehand to talk with the workers
and to ask them for their help. We had told them that we hoped to bring
disabled children from the government hostel (described earlier) so that
the course participants could evaluate their needs, and try to make them
simple assistive devices. The disabled shop-workers were eager to
assist. I had feared that a workshop with 60 participants would be
total chaos. The situation might be overwhelming for the disabled
children, especially those who were in delicate health. But my fears
were soon calmed. On arrival, the participants formed 6 groups, each
with a bewildered child. Among the participants were educators,
psychologists, physical and occupational therapists, technicians,
disabled persons, and - most important - mothers of disabled children.
The mothers, especially, tried to gain the children's confidence,
talking gently to them, then tenderly beginning to touch them and take
them into their arms. The children, starved for human contact, began to
smile and respond. Three participants with experience in evaluating
children's needs and in designing assistive equipment, circulated from
group to group offering assistance. At first, some participants were
afraid to rely on their own observations, or to innovate. But the
children's needs were so enormous that the groups started to improvise.
The disabled shop-workers - used to building wheelchairs and walkers -
began enthusiastically working on innovative designs. They assisted the
different groups when their skills were needed.
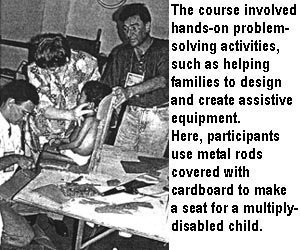
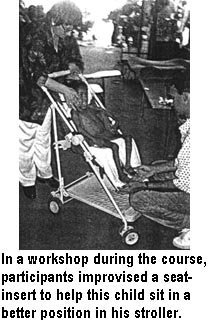
The results were impressive. Using cardboard, sticks, cloth, and bits
of tubing, the groups created a variety of useful assistive devices.
They made special seats, wheelchair inserts, supports for
improving body position and head control, a splint for better hand
function, tray tables, and colorful toys to hang above
a child to develop hand-eye coordination. The children seemed
to like both the attention and equipment. The staff from the hostel were
thrilled with the creativity. They said they would make equipment for
other children, and were delighted to receive a copy of Disabled
Village Children (in Portuguese) to provide ideas and guidelines.
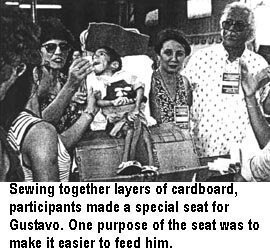
A survival seat for GUSTAVO. One of the children
whose needs were most critical was Gustavo. Completely paralyzed by
brain damage, the boy had been abandoned by his parents and ended up at
the government hostel. Skin and bones, at age 14 he looked about 6 years
old. Feeding him was hard, because his body and head were floppy and he
had little mouth control. Although he could not to move or speak, his
mental ability seemed intact. He could communicate only with his eyes.
But he appeared to understand most questions. He would close his eyes to
say no, and leave them open to say yes. At times, he almost smiled.
Gustavo seemed to like both his new seat and all the attention. But
sometimes when participants asked him questions, tears would roll down
his checks - as if he were frustrated at not being able to communicate
more effectively.
The participants realized that, although they were perhaps able to
help Gustavo in a small way - such as a seat that would make feeding him
easier - a lot remained undone. Gustavo needed a real home, a loving
family, public assistance, and community support. "I never knew there
were children like Gustavo in Brazil," said one rehabilitation center
coordinator, tears in her eyes. "So starved! So neglected! And in our
own institutions! How many more like him are there in Brazil?" |
| 336
|
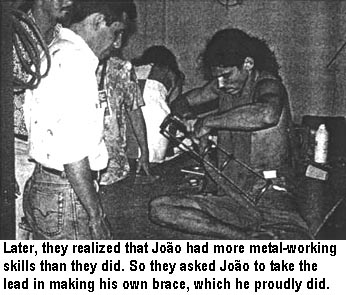
JOÃO, the shop worker.
João, a young metal worker in the wheelchair shop, had one of his
legs paralyzed by polio. He wanted to know if anything could be done so
he could walk without having to push his thigh with his hand. A group of
course participants tried to help João solve his problem. The group was
encouraged to work with João as an equal in the problem-solving process,
and not simply to design and make an assistive device for him.
"Work with him as a partner, not a patient!"
Examining João's leg, the group found that he had a knee contracture
of about 25 degrees which, if possible, needed to be corrected before
João tried to walk with a brace. They did a test to find out whether the
contracture was primarily in the muscles or in the knee itself (see
page 127). If the contracture is in the
muscles, it can often be corrected with exercise, casting, or bracing,
to slowly stretch the tight muscles. If the contracture is in the joint
capsule, surgery may be necessary.
To explain all this to João, the group used a life-sized
plywood skeleton made in Mexico (see
Chapter 20), which I had taken with me to Brazil. João enjoyed the
demonstration with the skeleton, and said it helped him to understand
the functions of his knee.
The group decided that the first step toward improving João's walking
was to make a night brace to gradually correct his knee
contracture. Among the course participants was an orthotist
(professional brace maker) who helped João's group design a simple leg
brace which they could make from two long, flat metal bars joined by
curved sections of metal tube (materials that were available in the
wheelchair shop).
João was the only person in his group with the metal-working skills
needed for making the brace. But when the group of professionals started
working, the predictable thing happened. João was left sitting on the
examining table, while the others began to cut, measure, and attempt to
bend the pieces for the brace. João watched passively without comment.
Then suddenly, one of the disabled participants woke up and said, "Hey!
João is more skilled at metal-work than we are. And he knows more about
his own leg. Rather than our making the brace for him, he should be
making it himself, with our help. That way, if he has to adjust or
re-make it after we are gone, he'll know how." Everyone agreed. With a
grin, João climbed off the table and took charge.
João did an excellent job of making his brace. Everyone learned a
great deal. But the most important lesson they learned was to
work with a disabled person as a partner and not a patient.
This is the key to enabling community rehabilitation.

|
| 337
|
CHILD-TO-CHILD: A MENTALLY HANDICAPPED GIRL LEARNS TO CARE FOR
MULTIPLY-DISABLED CHILDREN

The course participants were deeply concerned about the inadequate
care that disabled children at the hostel were receiving. They realized
that the care-providers at the hostel were overworked. "The hostel
desperately needs more staff, more help! Children are starving because
they don't have enough attendants to feed them! In the current economic
climate, the government cuts back on budgets for public services, even
as the need grows. What can be done?"
IDEA! Then an idea came. Next-door to this
hostel (part of the same institution) was a "home" for 50 abandoned
mentally-handicapped girls. The girls were taught daily living skills,
and many attended normal school (a big step forward). Some were also
taught work skills. But as the girls got older, many had no place to go.
So they stayed in the home with little direction or purpose in their
lives.
A possible solution to the needs of both hostels was
evident. One hostel needed more staff to help hold, hug, feed, and
mother the multiply-disabled children. The other hostel had mentally
slow girls with motherly instincts, who needed worthwhile activities.

Then why not invite the older, more capable
mentally-handicapped girls to help feed and care for the severely
disabled children?
Following up on this suggestion, on the second day of the CBR
workshop, caretakers from the government hostel brought one of the
older, more capable mentally-handicapped girls along with the 5
multiply-disabled children. The girl, MARÍA, was eager
to help. One of the course participants, herself a mother of a disabled
child, showed María how to hold and handle EMA, a small
girl with cerebral palsy who had almost no body control: María soon
learned how to position and feed Ema in her new special seat (made by
course participants). Another participant, a therapist, showed María how
to help the child develop head control - by holding her upright and
gently supporting the back of her head with her hands (see
page 37).
Follow up. Everyone agreed that a big achievement of
the course was the realization that a mentally slow girl like María
could provide a vital service by caring for disabled children. Two
course participants from Recife, a therapist and a priest, offered to
visit the hostel regularly to help train María and other girls, and to
assure that this Child-to-Child initiative is sustained. |
| 338
|
Old Plastic Buckets Have Many Uses
Davidcillo is the son of Magui, who has severe arthritis and runs the
cooperative village store in the village of Ajoya. PROJIMO often
provided child care for the baby while his mother tended the store. (See
the photos of Martín holding and bathing Davidcillo on pages
22 and 236.)
The baby was named after the author.
|
|